Fill Out a Valid Nevada Medicaid Redetermination Template
Fill Out a Valid Nevada Medicaid Redetermination Template
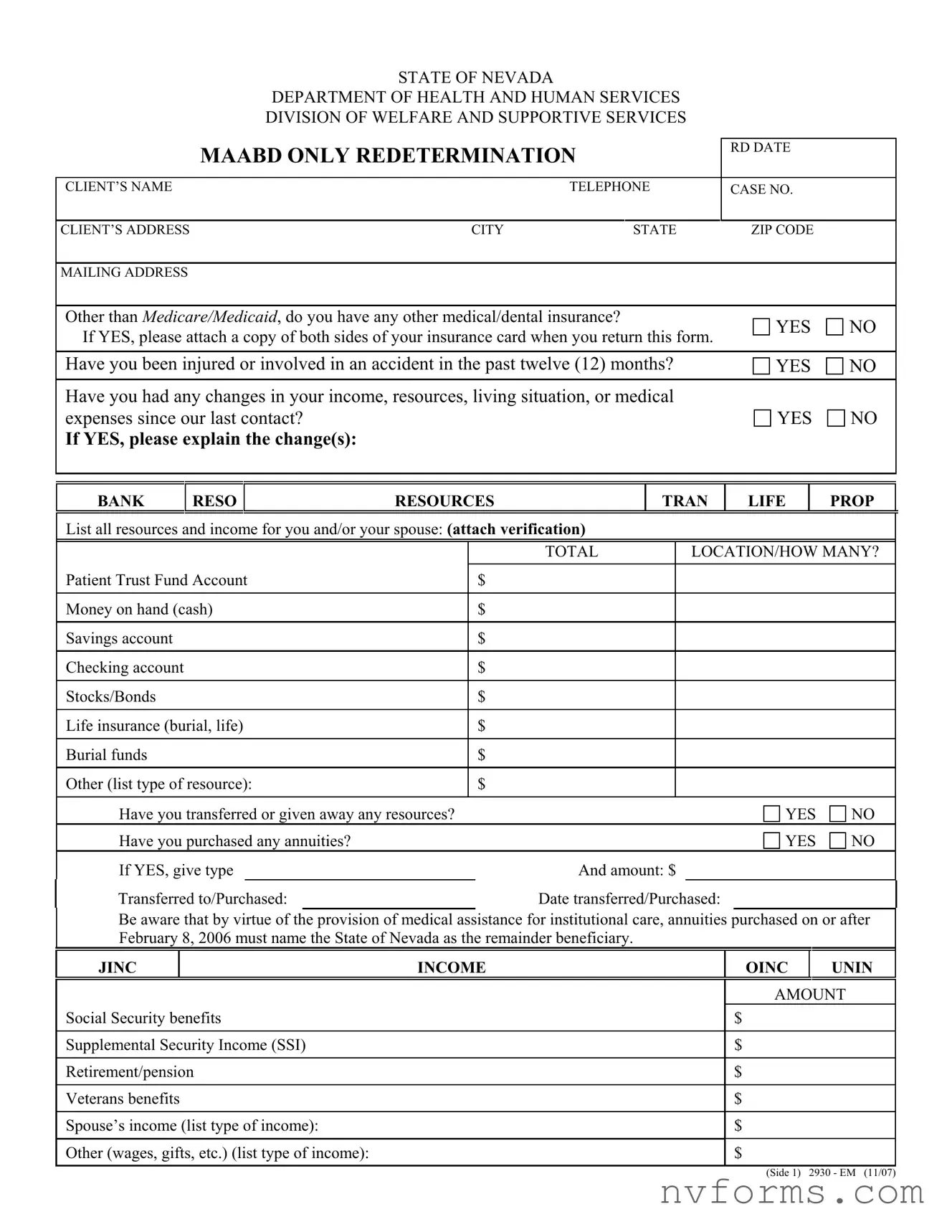
In Nevada, the process of maintaining Medicaid eligibility involves a thorough and detailed review, encapsulated in the Nevada Medicaid Redetermination form. Distributed by the Division of Welfare and Supportive Services, this document plays a crucial role in the lives of many, serving as a conduit for updates and changes that may affect Medicaid eligibility and coverage. It meticulously collects information ranging from the client's basic details to more specific inquiries such as additional medical or dental insurances, recent accidents or injuries, and any shifts in income, resources, living arrangements, or medical expenses. The form delves into a comprehensive list of personal and spouse's incomes, assets, and even accounts for changes not previously detailed. Moreover, it emphasizes the importance of naming a state as a remainder beneficiary for annuities purchased, a clear illustration of its thoroughness in ensuring the state's financial interests are safeguarded. Individuals are also reminded of their ongoing responsibilities under Medicaid, including the provision of Social Security Numbers for all household members seeking assistance, underscoring the intertwining of federal regulations and personal accountability in the maintenance of Medicaid benefits. This form is a stark reminder of the rigorous process individuals undergo to maintain their health coverage, reflecting both the bureaucratic aspects of public assistance and the deeply personal impact of such programs on individuals and their families.
STATE OF NEVADA
DEPARTMENT OF HEALTH AND HUMAN SERVICES
DIVISION OF WELFARE AND SUPPORTIVE SERVICES
MAABD ONLY REDETERMINATION |
|
RD DATE |
|
||
|
|
|
|||
|
|
|
|
||
CLIENT’S NAME |
TELEPHONE |
CASE NO. |
|
||
|
|
|
|
|
|
CLIENT’S ADDRESS |
CITY |
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
||
Other than MEDICARE/MEDICAID, do you have any other medical/dental insurance? |
|
YES |
NO |
||
If YES, please attach a copy of both sides of your insurance card when you return this form. |
|||||
|
|
||||
|
|
|
|||
Have you been injured or involved in an accident in the past twelve (12) months? |
YES |
NO |
|||
|
|
|
|||
Have you had any changes in your income, resources, living situation, or medical |
|
|
|||
expenses since our last contact? |
|
|
YES |
NO |
|
If YES, please explain the change(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BANK
RESO
RESOURCES
TRAN
LIFE
PROP
List all resources and income for you and/or your spouse: (attach verification)
|
|
|
|
TOTAL |
|
LOCATION/HOW MANY? |
|
|
|
|
|
|
|
|
|
Patient Trust Fund Account |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Money on hand (cash) |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Savings account |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Checking account |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Stocks/Bonds |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Life insurance (burial, life) |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Burial funds |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Other (list type of resource): |
$ |
|
|
|
|||
|
|
|
|
|
|
|
|
Have you transferred or given away any resources? |
|
|
|
YES |
NO |
||
Have you purchased any annuities? |
|
|
|
YES |
NO |
||
If YES, give type |
|
|
And amount: $ |
|
|
||
Transferred to/Purchased: |
|
|
Date transferred/Purchased: |
|
|||
Be aware that by virtue of the provision of medical assistance for institutional care, annuities purchased on or after February 8, 2006 must name the State of Nevada as the remainder beneficiary.
JINC
INCOME
OINC
UNIN
Social Security benefits
Supplemental Security Income (SSI)
Retirement/pension
Veterans benefits
Spouse’s income (list type of income):
Other (wages, gifts, etc.) (list type of income):
AMOUNT
$
$
$
$
$
$
(Side 1) 2930 - EM (11/07)
RENT
INCOME
SPOUSAL LIVING EXPENSES
UTIL
Shelter expenses (rent, mortgage, taxes, insurance, utilities)
List type of expense(s):
AMOUNT
$
$
$
AREP
MEDICAL EXPENSES
MEDX
Insurance premiums (list type of insurance): |
TOTAL AMOUNT/VALUE |
PAYMENT FREQUENCY |
|
|
|
|
$ |
|
|
|
|
Client medical bills (not payable by Medicaid): |
$ |
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
$ |
|
|
|
|
If you have had other changes not described above, please describe them in the area below. If you (or your spouse) are receiving any additional income or resources not listed on this form, please list them below and attach verification. If you want to name an authorized representative (A/R), or you want to name a different person as your A/R, please check this box 
 . Your case manager will send you a document to record your request. It must be completed and returned before your representative will be acknowledged on your case.
. Your case manager will send you a document to record your request. It must be completed and returned before your representative will be acknowledged on your case.
RIGHTS, RESPONSIBILITIES AND PENALTIES
At the time of your application, you signed a copy of your rights and responsibilities. These requirements continue to apply. You may contact your local office for a copy of these provisions.
Federal regulations now require Social Security Numbers (SSNs) for all individuals receiving or seeking to receive assistance for themselves. If you or an individual in your household is applying for assistance and do not wish to provide or apply for an SSN, only this person’s request for assistance will be denied. Undocumented or ineligible
DECLARATION AND SIGNATURE(S)
I/We have read (or had explained to me/us) and understand the information on both sides of this eligibility review form. I/We declare under the penalty of perjury, information I/we gave in this review is true, correct and complete to the best of my/our knowledge.
NOTE: Failure to return this form will affect your eligibility for benefits.
SIGNATURE OF CLIENT
TELEPHONE NUMBER
DATE
SIGNATURE OF AUTHORIZED REPRESENTATIVE
TELEPHONE NUMBER
DATE
CASE MANAGER SIGNATURE
DATE
(Side 2) 2930 - EM (11/07)
| Fact | Detail |
|---|---|
| Governing Law | Federal regulations and state laws pertaining to Medicaid in Nevada |
| Purpose of the Form | To reassess eligibility for MAABD (Medical Assistance for Aged, Blind, and Disabled) benefits |
| Information Required | Client identification, medical/dental insurance details, changes in financial situation, and declaration of rights, responsibilities, and penalties |
| Special Note on Annuities | Annuities purchased on or after February 8, 2006, must name the State of Nevada as the remainder beneficiary for individuals receiving institutional care |
| Requirement for Social Security Numbers | SSNs are required for verification of family’s income and resources, and to ensure no duplicate benefits are received |
When it's time to fill out the Nevada Medicaid Redetermination form, it's crucial to do so accurately to ensure your benefits continue without interruption. This form helps assess any changes in your circumstances that could affect your Medicaid eligibility. Follow the below steps to complete the form properly, attach any required documents, and return it by the specified deadline.
Once you've filled out the form and attached any necessary documents, return it to the specified address or office. Timely submission is important to avoid any disruptions in your Medicaid coverage. Should you have any questions or need assistance, do not hesitate to contact your case manager or the local office.
Welcome to the FAQ section on the Nevada Medicaid Redetermination form. This guide is designed to address common questions and concerns, helping ensure individuals have the necessary information to complete and submit their forms accurately. The goal is to assist in maintaining Medicaid benefits without interruption.
The Nevada Medicaid Redetermination form is a document used by the State of Nevada Department of Health and Human Services, Division of Welfare and Supportive Services, to reassess eligibility for Medicaid benefits. It is crucial for ensuring that individuals who require medical assistance continue to receive the support they need based on current information regarding their income, resources, living conditions, and medical expenses.
Completing and returning the Redetermination form is vital because it directly affects your eligibility for Medicaid benefits. Failure to submit the form could result in the termination of benefits. It ensures that the information on file is up to date and that you or your spouse receive the appropriate level of assistance.
If you have other medical or dental insurance, it is important to indicate this on the Redetermination form and attach a copy of both sides of your insurance card. This allows for accurate coordination of benefits and ensures that Medicaid can work effectively with your other insurance providers.
Any changes in your income, resources, living situation, or medical expenses should be clearly explained in the designated section of the form. It is also necessary to attach verification for all listed resources and income for you and/or your spouse. Accurate reporting helps determine the correct level of benefits you are eligible for.
If you have purchased annuities, you must disclose the type and amount on the form. Since February 8, 2006, annuities purchased for medical assistance for institutional care must name the State of Nevada as the remainder beneficiary. This requirement is part of the Medicaid eligibility criteria and helps protect the state's interest.
If you've had changes not specifically listed on the form, describe them in the provided space. This could include additional income, resources not mentioned, or any other significant changes affecting your eligibility. Providing complete information ensures accurate assessment of your situation.
To name or change an authorized representative, check the appropriate box on the form. Your case manager will send you a document to record your request, which must be completed and returned. An authorized representative can act on your behalf regarding your Medicaid case, providing an extra layer of support.
Your rights and responsibilities were detailed at the time of your application and continue to apply throughout your participation in the Medicaid program. You may contact your local office to receive a copy of these provisions, which include compliance with program requirements and the importance of providing accurate and truthful information.
SSNs are required for all individuals receiving or seeking to receive assistance to verify family income and resources. They are used in computer matching with other agencies, investigations, and to prevent duplication of benefits. Providing your SSN is essential for maintaining transparency and eligibility for Medicaid benefits.
This FAQ aims to clarify the purpose and importance of the Nevada Medicaid Redetermination form, highlighting key components and requirements. Accurately completing and returning this form is crucial for continuing to receive Medicaid benefits and ensuring your health and well-being.
Filling out the Nevada Medicaid Redetermination form is a critical step to ensure that individuals continue to receive their Medicaid benefits without interruption. However, errors during the completion process are not uncommon. Recognizing and avoiding these mistakes can be pivotal in facilitating a smooth review process. Below are six common pitfalls encountered by applicants:
Not providing updated information. It’s imperative that all changes in income, resources, living situation, or medical expenses since the last verification are reported accurately. Failing to mention these updates can lead to incorrect eligibility determination.
Omitting additional insurance details. If an applicant has other medical or dental insurance besides Medicare/Medicaid, the form requires a copy of both sides of the insurance card. Neglecting to attach this documentation can delay the review process.
Incorrect or incomplete financial information. The form asks for detailed information about income and resources. This includes bank accounts, life insurance, stocks, bonds, and more. Inaccuracy or failure to disclose these resources can impact Medicaid eligibility.
Forgetting to name the State of Nevada as the remainder beneficiary. For annuities purchased after February 8, 2006, it's a requirement to name the State of Nevada as the remainder beneficiary if applying for Medicaid for institutional care. Missing this detail can affect the acceptance of the application.
Failure to report changes in household composition. Any shifts, such as those in the number of dependents or living arrangements, can affect eligibility and must be reported. Overlooking this requirement can lead to inaccurate benefit calculations.
Leaving the authorized representative section blank. Designating an authorized representative can be crucial, especially for individuals who might need assistance in managing their Medicaid benefits. Not taking the time to complete this section can hinder communication between Medicaid and the individual.
Several steps can be taken to avoid these common mistakes:
Avoiding these mistakes not only accelerates the redetermination process but also ensures that individuals receive the correct level of benefits without unnecessary interruption. It underscores the importance of attention to detail and staying informed about the requirements of the Nevada Medicaid program.
When it comes to maintaining healthcare benefits through Nevada Medicaid, the Redetermination form is a crucial document that helps determine continued eligibility based on current circumstances. However, completing this process often requires additional documentation to verify the information provided. These auxiliary documents ensure that the Department of Health and Human Services has a comprehensive understanding of an individual's or family’s financial and living situation, thereby making accurate eligibility determinations.
Individuals seeking to maintain their Nevada Medicaid coverage should gather these documents promptly to accompany their Redetermination form. By providing complete and accurate information supported by the appropriate documents, applicants can facilitate a smoother review process, helping ensure their eligibility is assessed correctly and efficiently. Remember, the goal is to maintain continuous coverage and access to vital healthcare services, and preparing these documents in advance can make a significant difference.
The Nevada Medicaid Redetermination form is similar to Annual Income Tax Return forms, such as the IRS Form 1040. Both require detailed financial information, including income, deductions, and applicable credits. The Medicaid form, like the tax return, asks for income from various sources such as Social Security benefits, retirement/pension, and any other wages or gifts. Both forms require individuals to declare their financial status accurately, under penalty of perjury. While the tax form focuses on calculating tax liability or refunds, the Medicaid form assesses eligibility for medical assistance based on financial status.
This form also shares similarities with General Insurance Application forms. Both ask about other insurance coverages you might have, requiring details of any medical or dental insurance outside of Medicaid/Medicare. Importantly, both necessitate the attachment of insurance cards or policy documents for verification, just as insurance applications often require proof of prior insurance or health statements. They both play a critical role in determining your coverage scope - in the case of Medicaid, to ensure primary and secondary insurance coverages are correctly coordinated.
Lastly, the form resembles Financial Aid Application forms used for educational purposes, such as the FAFSA (Free Application for Federal Student Aid). Both delve into the financial aspects of an individual’s or family’s income and resources, including bank accounts, stocks, bonds, and other assets. They ask about changes in financial circumstances that could affect eligibility or the amount of aid offered. Furthermore, both forms emphasize the significance of accurate and truthful reporting of financial information, with implications for misreporting or failure to provide required documentation.
When tackling the Nevada Medicaid Redetermination form, there are specific actions you should take to ensure the process goes smoothly and avoid common pitfalls. Here's a guide to help you complete the form effectively:
Do:
Don't:
When it comes to Medicaid Redetermination in Nevada, there are several misconceptions that can lead to mistakes or missed opportunities. It's crucial to have the right information to successfully navigate this process.
Misconception 1: You only need to complete the redetermination form if your circumstances have changed. Actually, even if nothing has changed, you must still complete and return the form to ensure your Medicaid coverage continues without interruption.
Misconception 2: You don’t need to report all types of income or resources. In truth, the form requires you to list all income and resources, not just the ones you think are relevant. This includes both earned and unearned income, as well as any resources you or your spouse may have.
Misconception 3: If you have other medical or dental insurance, it doesn’t affect your Medicaid. This is inaccurate. You need to inform Medicaid of any other insurance coverage, as it can affect your eligibility or the way your benefits are calculated.
Misconception 4: Reporting an accident or injury is unnecessary. On the contrary, it’s important to report any accidents or injuries since Medicaid may need to coordinate benefits if there's another party responsible for covering medical costs.
Misconception 5: Providing Social Security Numbers (SSNs) for household members is optional. SSNs are actually required for anyone applying for assistance, as they are used to verify income, resources, and to prevent duplicative benefits.
Misconception 6: You can have someone else act on your behalf without formally designating them. To have a representative manage your Medicaid affairs, you must officially name them on the form and submit the necessary documentation to recognize this arrangement formally.
Misconception 7: Transferred or gifted resources do not need to be reported. Contrary to this belief, you must disclose any transferred or given away resources as these can impact your eligibility, specifically for long-term care benefits.
Misconception 8: Annuities do not affect Medicaid eligibility. If you have purchased any annuities, they must be reported, and the State of Nevada should be named as the remainder beneficiary for annuities purchased after February 8, 2006, to comply with eligibility requirements.
Misconception 9: It’s okay to estimate income and resource values. Accurate information is essential. Estimations can lead to incorrect eligibility determinations and may result in penalties, including repayment of benefits or legal consequences.
Having correct and detailed information when completing the Nevada Medicaid Redetermination form is vital. Avoiding these common misconceptions can help you maintain continuous coverage and access to health care benefits.
Filling out the Nevada Medicaid Redetermination form is an important process for maintaining your Medicaid coverage. Here are ten key takeaways to guide you through this process:
Remember, failing to return this form or providing incomplete or inaccurate information could affect your eligibility for benefits. Read and understand your rights, responsibilities, and the penalties for false declarations carefully. Social Security Numbers are required for verification purposes and to prevent duplication in benefits. Sign the declaration to confirm that all the information provided is true and complete to the best of your knowledge.
Nevada Check Up Income Limits 2023 - Applicants are asked to provide detailed information about all adults and children in the household, including citizenship status, which is treated with confidentiality and not reported to INS.
Free Paternity Test Las Vegas - The declaration includes a 60-day period during which the paternity acknowledgment can be revoked, emphasizing the importance of thoughtful consideration before signing.
Nevada Medicaid Eligibility Check - The structured format of the form supports clear and organized presentation of necessary information, enhancing the efficiency of the authorization review process.