Fill Out a Valid Universal Referral Nevada Template
Fill Out a Valid Universal Referral Nevada Template
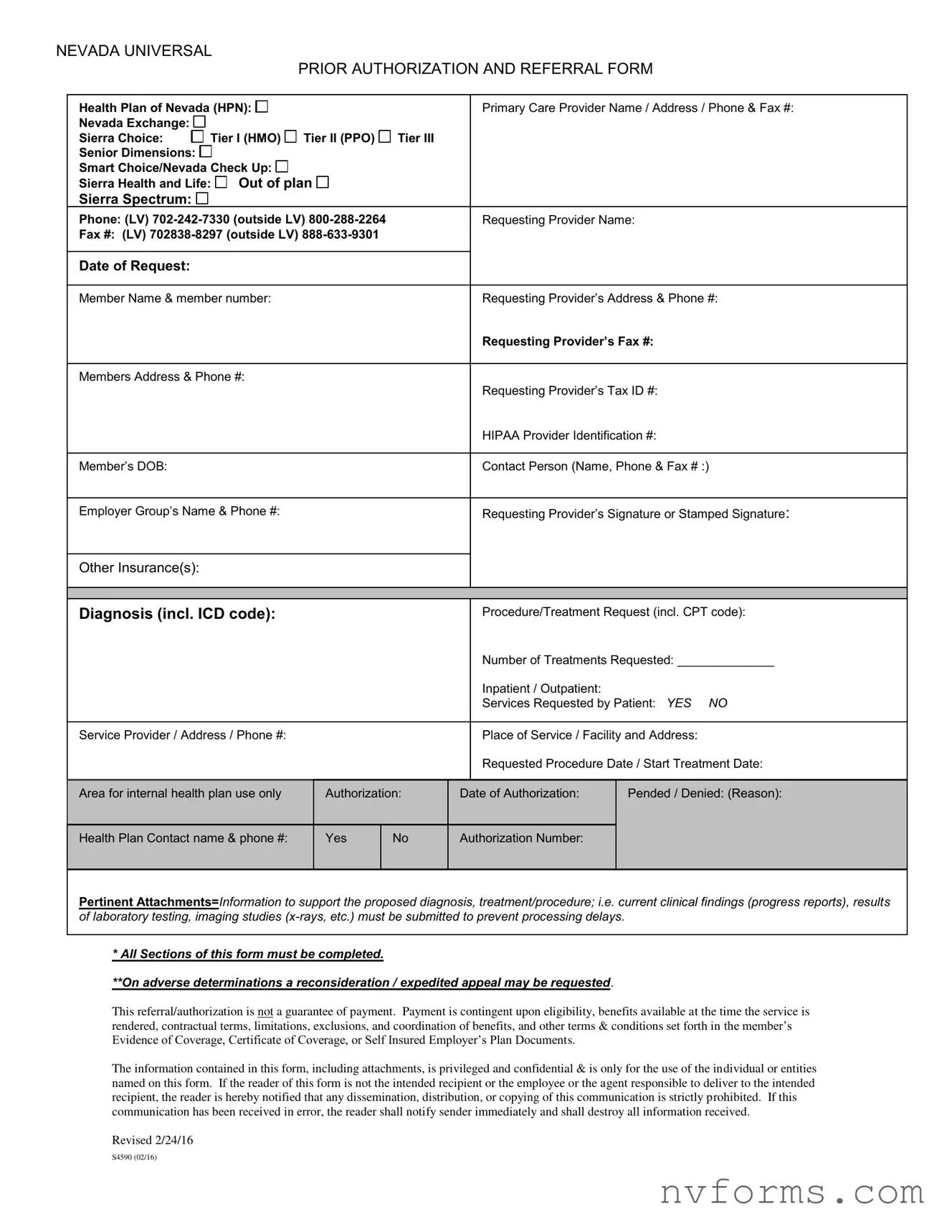
In Nevada, navigating the complexities of health insurance referrals and prior authorizations is streamlined through the introduction of the Universal Referral Nevada form. This comprehensive document is a critical tool utilized by healthcare providers to coordinate and streamline patient care among various health plans, including Health Plan of Nevada (HPN), Nevada Exchange tiers, Sierra Choice, Senior Dimensions, and others. It captures essential details such as the primary care provider's contact information, the requesting provider’s details, member information, diagnosis, proposed treatments or procedures, and the necessary insurance data to effectively process the request. The form mandates the inclusion of clinical findings and might require attachments to support the diagnosis and proposed treatment plans, with the aim of minimizing processing delays. Notably, the form is also a medium through which providers can request a reconsideration or expedited appeal in cases of adverse determinations. However, it emphasizes that the authorization or referral granted through this form does not guarantee payment, as actual payment is contingent upon several factors including eligibility, benefit availability, and adherence to contractual terms and plan documents. It also highlights the confidential nature of the information contained within, stressing its limited use to the individuals or entities specified. With its last revision on February 24, 2016, this form stands as an essential part of healthcare administration in Nevada, facilitating a smoother, more coordinated approach to patient care across different health services and insurance plans.
NEVADA UNIVERSAL
PRIOR AUTHORIZATION AND REFERRAL FORM
Health Plan of Nevada (HPN): |
|
|
|
|
|
|
|
|
|
|
|
|
Primary Care Provider Name / Address / Phone & Fax #: |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||
Nevada Exchange: |
|
|
|
|
|
Tier I (HMO) |
|
|
Tier II (PPO) |
|
Tier III |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Sierra Choice: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||
Senior Dimensions: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Smart Choice/Nevada Check Up: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Sierra Health and Life: |
|
|
Out of plan |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||
Sierra Spectrum: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Phone: (LV) |
|
|
Requesting Provider Name: |
|||||||||||||||||||||
Fax #: (LV) |
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Date of Request: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Member Name & member number: |
|
|
|
|
|
|
|
Requesting Provider’s Address & Phone #: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Requesting Provider’s Fax #: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Members Address & Phone #: |
|
|
|
|
|
|
|
Requesting Provider’s Tax ID #: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HIPAA Provider Identification #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Member’s DOB: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Contact Person (Name, Phone & Fax # :) |
||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Employer Group’s Name & Phone #: |
|
|
|
|
|
|
|
Requesting Provider’s Signature or Stamped Signature: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Other Insurance(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Diagnosis (incl. ICD code): |
|
|
|
|
|
|
|
Procedure/Treatment Request (incl. CPT code): |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of Treatments Requested: ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inpatient / Outpatient: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Services Requested by Patient: YES NO |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Service Provider / Address / Phone #: |
|
|
|
|
|
|
|
Place of Service / Facility and Address: |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Requested Procedure Date / Start Treatment Date: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||
Area for internal health plan use only |
|
|
Authorization: |
|
|
|
||||||||||||||||||
|
|
Date of Authorization: |
Pended / Denied: (Reason): |
|||||||||||||||||||||
CURRENT CLINICAL FINDINGS AND |
MANAGEMENT |
|
use the space – also see requirements below and attach to this form. |
|||||||||||||||||||||
All procedures/treatment requested require |
clinical information (may |
|||||||||||||||||||||||
Health Plan Contact name & phone #: |
|
|
Yes |
|
No |
Authorization Number: |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*All sections of this form must be completed.
Pertinent Attachments=Information to support the proposed diagnosis, treatment/procedure; i.e. current clinical findings (progress reports), results
of laboratory testing, imaging studies
**On adverse determinations a reconsideration / expedited appeal may be requested.
* All Sections of this form must be completed.
**On adverse determinations a reconsideration / expedited appeal may be requested.
This referral/authorization is not a guarantee of payment. Payment is contingent upon eligibility, benefits available at the time the service is rendered, contractual terms, limitations, exclusions, and coordination of benefits, and other terms & conditions set forth in the member’s Evidence of Coverage, Certificate of Coverage, or Self Insured Employer’s Plan Documents.
The information contained in this form, including attachments, is privileged and confidential & is only for the use of the individual or entities named on this form. If the reader of this form is not the intended recipient or the employee or the agent responsible to deliver to the intended recipient, the reader is hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited. If this communication has been received in error, the reader shall notify sender immediately and shall destroy all information received.
Revised 2/24/16
S4590 (02/16)
| Fact | Details |
|---|---|
| Governing Law(s) | N/A - Specific laws governing the use of this form are not listed, but it operates under Nevada state healthcare regulations and federal HIPAA privacy standards. |
| Intended Use | For requesting prior authorization and referrals within various health plans including Health Plan of Nevada (HPN), Sierra Choice, Senior Dimensions, Smart Choice/Nevada Check Up, and Sierra Health and Life. |
| Completion Requirement | All sections of the form must be completed to prevent processing delays. Pertinent attachments supporting the diagnosis and treatment plan are required. |
| Key Contact Information | Includes contact details for both the requesting provider and the health plan, to facilitate easy communication and processing of the request. |
| Guarantee of Payment | The form explicitly states that completing and submitting it is not a guarantee of payment. Payment depends on eligibility, available benefits, contractual terms, and other conditions listed in membership documents. |
| Confidentiality Notice | The information provided in the form is confidential and intended only for the use of the individual or entity named on the form. Unauthorized sharing is strictly prohibited. |
Upon receiving the Universal Referral Nevada form, it is crucial for both the requesting provider and the member seeking services to fill it out with accuracy and thoroughness. This form is a key step in facilitating the processing of a service request through the specific health plan, and ensuring all information is correctly provided will assist in reducing processing times and avoid any unnecessary delays. Here is a stepwise guide on how to complete the form:
After completing all the required sections of the form, make sure to attach any Pertinent Attachments such as current clinical findings, progress reports, results of laboratory testing, or imaging studies to support the diagnosis and proposed treatment or procedure. Timely and comprehensive completion of this form, including necessary attachments, is crucial for facilitating the referral process.
Please note that the submission of this form does not guarantee payment. Payment depends on various factors including eligibility, benefits available at the time the service is rendered, and adherence to contractual terms and conditions. Additionally, in the case of adverse determinations, a reconsideration or expedited appeal process may be requested. It's essential to retain a copy of this form and all communications for your records. Remember, confidentiality and accuracy in handling this form are imperative.
What is the Universal Referral Nevada Form?
The Universal Referral Nevada Form is a standardized document used across various health plans in Nevada for processing prior authorizations and referrals. It collects comprehensive information about the patient, the requesting provider, the type of coverage, the requested service, and supports the information with clinical findings. The form is designed to streamline the process of requesting and authorizing medical procedures and treatments.
Who should complete the Universal Referral Nevada Form?
This form should be completed by the healthcare provider requesting a referral or prior authorization for a patient's treatment or procedure. It requires detailed information, including both the requesting provider's and the patient's identifiers, diagnosis, proposed treatment, and insurance coverage details. All sections of the form must be fully completed to avoid delays in processing.
What information is required on the form?
The form requires several pieces of information, such as:
In addition, the form must include any other insurance information and a detailed description of the current clinical findings and the management plan.
Is completion of the Universal Referral Nevada Form a guarantee of payment?
No, completing and submitting the Universal Referral Nevada Form is not a guarantee of payment. Payment depends on factors such as eligibility, benefits available at the time the service is rendered, contractual terms, limitations, exclusions, coordination of benefits, and other terms & conditions outlined in the member’s Evidence of Coverage or Plan Documents. This serves as an authorization tool and not a promise of coverage.
What should be done if a request is denied or requires reconsideration?
If a request is denied or requires reconsideration, the form outlines a process for requesting a reconsideration or an expedited appeal. This involves reviewing the adverse determination and, if necessary, submitting additional information or clarification to support the reconsideration or appeal. It is important to follow the specific instructions provided by the health plan regarding appeals to ensure proper handling and review of the case.
When it comes to filling out the Universal Referral Nevada form, attention to detail is crucial for ensuring that the referral or authorization request is processed efficiently and effectively. However, several common mistakes can create delays or even result in denials of requests. By understanding and avoiding these errors, individuals and healthcare providers can streamline the process and facilitate better health outcomes.
One of the most significant mistakes is incomplete information. All sections of the form must be filled out. This includes the Primary Care Provider's information, the Requesting Provider's details, the member's information, and the specifics of the diagnosis and requested procedure or treatment. Leaving any section incomplete can result in the delay of the referral or authorization process.
Incorrect or outdated member information is another common error. It's vital to double-check the member's name, member number, address, phone number, and date of birth. Any mismatch or outdated information can lead to processing delays or incorrect billing.
Failure to attach supporting documentation can be problematic. The form stipulates that current clinical findings, progress reports, and results from laboratory tests or imaging studies must accompany the request to avoid processing delays. Neglecting to attach these crucial pieces of evidence can lead to a lack of sufficient information for the request to be approved.
Lastly, omitting the Requesting Provider's signature or stamped signature is a mistake that can render the form invalid. This signature is necessary to authenticate the request and confirm that the provider has verified the information on the form. An unsigned form is unlikely to be processed until this oversight is corrected.
The Nevada Universal Prior Authorization and Referral Form is a critical document that facilitates a wide range of medical procedures and treatments. By ensuring that all information is accurate, complete, and properly documented, healthcare providers can help ensure that their patients receive the care they need without unnecessary delays. Remembering to review the form thoroughly before submission can significantly impact the efficiency of the processing and ultimately, the health outcomes for the member.
When handling the Universal Referral Nevada form, there are several additional forms and documents often required to ensure comprehensive and coordinated care for the patient. These documents aid in providing a complete picture of the patient's health needs and ensure that all necessary information is accurately communicated between providers.
Together, these documents support the referral process, ensuring that every healthcare provider involved has the necessary information to provide the best care possible to the patient. By meticulously gathering and sharing this information, healthcare providers can ensure a smooth transition and continuity of care for the patient.
The Universal Referral Nevada form is similar to various other documents used in the healthcare and insurance industries, each designed to streamline processes and improve patient care coordination. When examining its counterparts, the similarities in structure, intent, and function become evident, underscoring the form's importance in facilitating healthcare services.
Medical Referral Forms used by healthcare providers share a significant resemblance to the Universal Referral Nevada form. Like this form, medical referral forms typically include the referring provider's name, contact information, and the reason for the referral, encapsulated via diagnosis and treatment codes. They also require detailed information about the patient, such as their name, date of birth, and insurance details. The purpose behind both forms is to ensure the patient is referred to the appropriate specialist or service needed for their care, making the process as efficient as possible by including all pertinent information that the specialist or service provider might need.
Prior Authorization Forms in the healthcare industry are also akin to the Universal Referral Nevada form. These forms are necessary when a healthcare provider needs to obtain approval from a health insurance company before performing a specific procedure or prescribing a certain medication. They include comprehensive information about the patient, the provider, the diagnosis, and the proposed treatment or medication, similar to what is found on the Universal Referral Nevada form. The emphasis is on providing detailed clinical justification for the requested service or medication, resembling the section on the Nevada form where clinical findings and management details are outlined to support the diagnosis and proposed procedure or treatment.
Insurance Claim Forms, while primarily focused on the financial aspect of healthcare services, share some structural similarities with the Universal Referral Nevada form. These forms collect patient and provider information, details of the treatment or service provided, and the associated costs. The similarity lies in the granularity of information collected, including diagnosis and treatment codes, to ensure that the services provided are accurately documented and justified for insurance purposes. This comprehensive collection of information facilitates the processing of claims and helps in determining the eligibility for coverage, much like how the Universal Referral Nevada form aids in securing authorization for specific healthcare services.
Completing the Universal Referral Nevada form requires attention to detail and a clear understanding of the guidelines. Here are seven dos and don'ts to help you navigate the process efficiently and accurately.
Remember, accurately filling out the Universal Referral Nevada form is crucial for a streamlined referral process. Errors or omissions can not only cause delays but also impact the eligibility and coverage for the proposed services. Additionally, be mindful that an authorization is not a guarantee of payment. Payment depends on various factors, including eligibility, benefits available, and adherence to the terms set forth in the member’s coverage documents. Confidently navigate the form by adhering to these guidelines, ensuring a smoother process for both the provider and the patient.
There are several misconceptions regarding the Nevada Universal Referral and Authorization Form that need clarifying. This form is a crucial document within Nevada's healthcare system designed to streamline patient referrals and prior authorization processes, but misunderstandings can complicate its use.
Misconception 1: The form guarantees payment for services.
This is incorrect. The form itself does not guarantee payment. Payment is contingent upon various factors, including patient eligibility, the benefits available at the time service is rendered, and terms set forth in the member’s health plan.
Misconception 2: All healthcare plans utilize the same form.
While the form aims for universal application across different health plans in Nevada, specifics may vary slightly between different health plans, such as the Health Plan of Nevada (HPN) and Sierra Health and Life. It's essential to check for any plan-specific requirements.
Misconception 3: Approval is automatic upon submission.
Approval of a request is not automatic upon form submission. The request goes through a review process where the medical necessity and other factors are considered before an authorization decision is made.
Misconception 4: The form is only for inpatient treatment requests.
The form is used for both inpatient and outpatient treatment requests. This includes procedures, therapies, and other types of care a patient may need.
Misconception 5: All sections of the form are not mandatory.
Contrary to this belief, all sections of the form must be completed to avoid processing delays. Incomplete forms could delay or even result in denial of the authorization request.
Misconception 6: The form serves as a referral and authorization for any healthcare service.
The form is used specifically for services that require prior authorization. Not all healthcare services need prior authorization, and thus, not all services can be referred or authorized using this form.
Misconception 7: Patient consent is not necessary for the form's completion.
Patient consent is often required, especially in sharing their medical information among providers, to comply with privacy laws and regulations, including the Health Insurance Portability and Accountability Act (HIPAA).
Misconception 8: There is no need to attach additional documentation.
Additional documentation supporting the diagnosis, treatment, or procedure requested is essential. This may include progress reports, laboratory testing results, and imaging studies to support the case for authorization.
Misconception 9: The form covers multiple requests.
Each form typically covers a single request for treatment or procedure. Multiple requests may require separate forms, unless specified otherwise by the health plan.
Understanding the purpose, requirements, and correct usage of the Nevada Universal Referral and Authorization Form is important for healthcare providers to ensure smooth processing of patient referrals and authorizations for the necessary treatments or procedures.
Filling out the Universal Referral Nevada form correctly is crucial for ensuring timely and proper medical care coordination. Let's go over some key takeaways to help navigate this process efficiently.
By paying close attention to the details and requirements outlined in the Universal Referral Nevada form, providers can facilitate a smoother process for obtaining necessary medical services for their patients. Proper completion and understanding of this document are key steps in navigating the complexities of healthcare coordination and ensuring that patients receive the care they need.
Id Nevada - Mandates the signature of both the applicant and a DMV representative, ensuring mutual acknowledgment of the form's declarations and agreements.
Nevada Title Transfer Form - Nevada’s VP-254 guides the certification of motorcycles altered for road use, ensuring compliance with state safety inspections.
Dl 44 Form for Minors - Unpack the process of fulfilling the Nevada DMV’s requirements with the DLD-100 form for license renewal.